In a previous posting, I talked about controlling vertical growth problems by placing composite resin or glass ionomer cement on the occlusal surface of terminal molars. You can also place composite on the lingual of upper anterior teeth. How do you decide which to do? If you want to intrude molars (think open bite), use posterior turbos. If you want to extrude molars (think deep bite) use anterior turbos.

To bond these into place, you merely micro etch or pumice the lingual of the upper central incisors and then either traditional etch for 30 seconds or use a L-pop for 5 seconds. Place a generous amount of flowable composite on the custom turbo surface that faces the tooth. No bonding resin required.* Then place the custom turbo on the tooth. The cap insures that it is at the proper height. Do not etch the incisal 1 mm of the tooth so that the cap will be easy to remove.
*No sealant makes it easier to remove the cap at the end of this phase of treatment. If you are dealing with a deep bite particularly in a teenage male carnivore, use Assure or something similar to enhance bond strength.

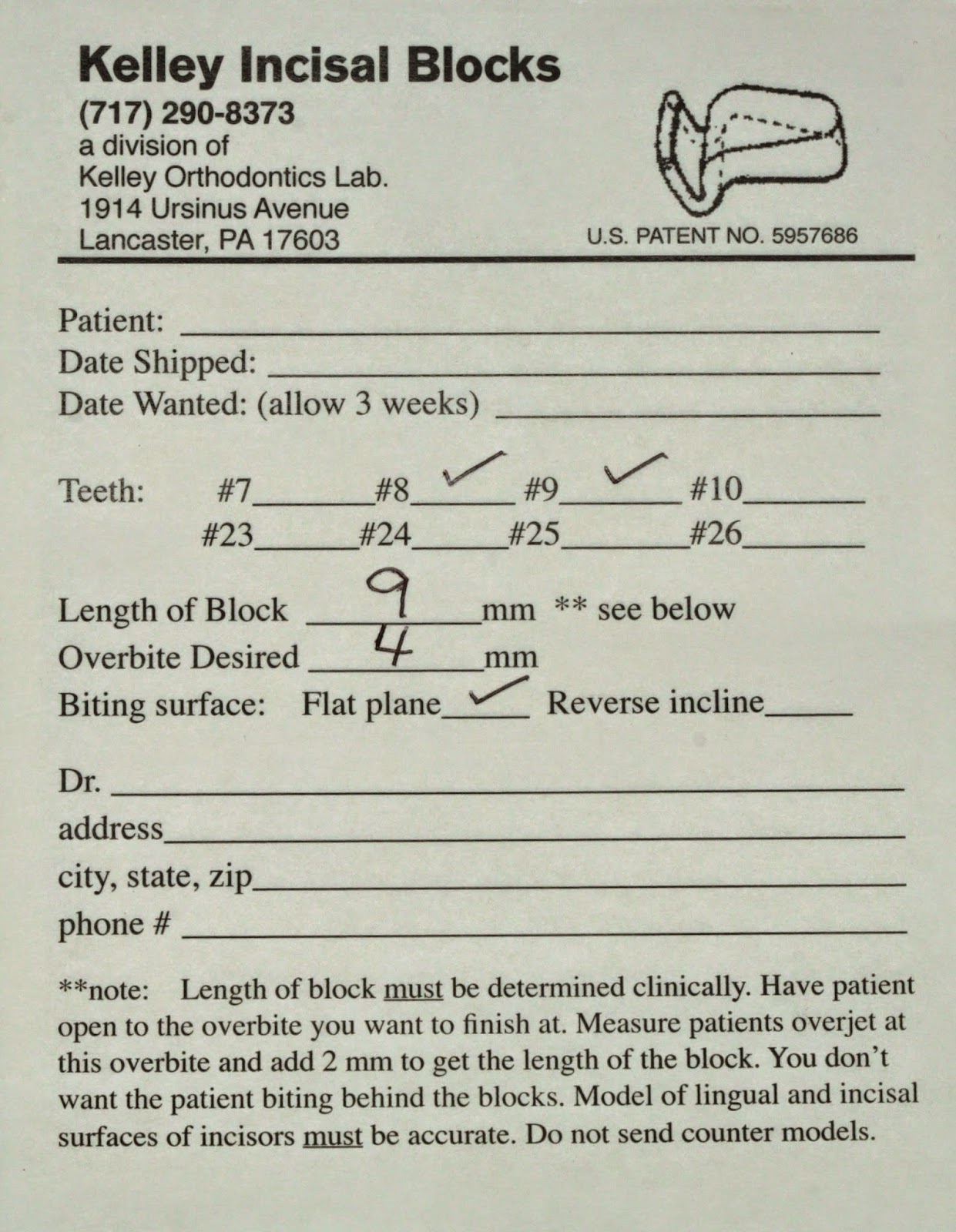
Light cure for 30 seconds. Then use a #8 round bur in a slow speed to remove the cap and to smooth out the lingual anatomy as necessary. You can advise light chewing for the next 24 hours but these things are pretty rugged and they rarely come off. Depending on your state laws, all of the above can be delegated. Finally, mark with blue paper and decide whether you need to full 9 mm or you can remove the excess with a straight diamond in a high speed.
In the photo below right, you can see I cut back on the length of the block. I usually leave the turbos in until I am in a full size lower working wire. For me that is a 19x25 in a 22 slot. So that usually means 6 months. You only have to grab the sides of the turbo with a How plier and squeeze once or twice to remove it. Typically this fractures the cement and the turbo comes off.
 Some people like to put these on during space closure if extractions were done or even in a deep bite non extraction case. By opening the bite, you facilitate tooth movement.
Some people like to put these on during space closure if extractions were done or even in a deep bite non extraction case. By opening the bite, you facilitate tooth movement.
Please make any comments or ask any questions below.


